
Dr. Alessandro Giardini

If you have been told that your child has a narrowing of the aorta (known as Aortic Coarctation), the main artery carrying blood from the heart to the body, it is completely understandable to feel concerned. The reassuring news is that coarctation of the aorta is a well-recognised congenital heart condition, and with modern treatment most children go on to lead completely normal, active lives. The key is understanding how significant the narrowing is and whether it is affecting the heart or circulation. In many cases, Dr Giardini can clarify this quickly during a single specialist appointment.
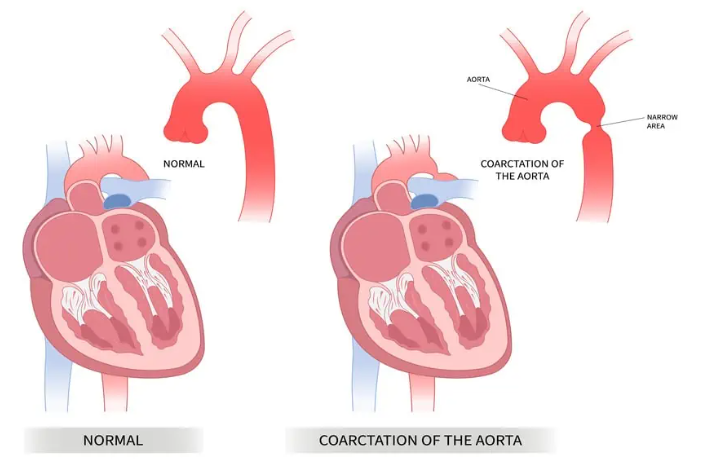
The aorta is the largest artery in the body. It rises from the left ventricle (the heart's main pumping chamber), arches over the top of the heart, and then runs downward through the chest and abdomen, supplying oxygen-rich blood to every organ and tissue. Coarctation of the aorta is a congenital narrowing of this artery, most commonly occurring just beyond the point where the artery to the left arm (the left subclavian artery) branches off.
Because of this narrowing, the heart has to work harder to push blood past the tight segment. Blood pressure becomes elevated in the upper body (head and arms) while blood flow to the lower body (abdomen, kidneys and legs) is reduced. Over time, the extra workload causes the left ventricle to thicken (a process called hypertrophy), and the elevated blood pressure in the upper body can place strain on the blood vessels.
The significance of these effects depends entirely on how tight the narrowing is. A mild coarctation may cause no symptoms for years and be discovered incidentally during a routine examination. A severe coarctation in a newborn baby can become a medical emergency in the first days of life. In between these two extremes, there is a wide spectrum, and a key part of Dr Giardini's assessment is determining exactly where your child sits on it.
Although the narrowing most commonly occurs in the classic position just beyond the left subclavian artery, coarctation can occasionally affect the aortic arch (the curved section at the top) or, more rarely, the abdominal aorta. In a small number of cases, a segment of the aorta may be completely interrupted rather than simply narrowed, a condition known as interrupted aortic arch, which requires early surgical repair.
Coarctation develops before birth during the formation of the heart and great vessels. In most cases, there is no identifiable cause, and nothing a parent did or did not do played any role. It affects approximately 4 to 6 in every 10,000 live births, accounting for around 6 to 8% of all congenital heart defects, and is more common in boys than girls.
There is a well-recognised association between coarctation and Turner syndrome, a genetic condition affecting girls in which one of the two X chromosomes is incomplete or missing. Coarctation can also run in families, and there are instances of multiple children in the same family being affected to varying degrees.
One of the most important associations is with bicuspid aortic valve. Up to 50 to 85% of children with coarctation also have an aortic valve with two leaflets instead of the normal three. A bicuspid valve may function normally for many years but can eventually develop narrowing (stenosis) or leakage (regurgitation), which is why long-term monitoring of both the aorta and the aortic valve is important. Coarctation can also occur alongside other congenital heart defects, including ventricular septal defects and patent ductus arteriosus.
Coarctation can sometimes be suspected on foetal echocardiography, although it is one of the more difficult congenital heart conditions to diagnose prenatally. Signs that may raise suspicion include a size difference between the left and right sides of the heart or narrowing of the aortic arch on the fetal scan. However, the fetal circulation is different from the circulation after birth, and the full extent of the narrowing may only become apparent once the baby is born and the ductus arteriosus closes.
If coarctation has been suspected prenatally, the baby will be monitored closely after delivery with echocardiography and clinical assessment. A prenatal suspicion does not always confirm the diagnosis, and some babies turn out to have a normal aorta after birth. Equally, some cases of coarctation are not apparent on fetal scanning and present after delivery. Dr Giardini can discuss the implications of a prenatal finding and arrange appropriate postnatal assessment.
Symptoms depend on the severity of the narrowing and the age at which it becomes apparent.
In newborn babies with a severe coarctation, the condition often presents in the first few days of life. During pregnancy, the ductus arteriosus (a normal fetal blood vessel connecting the pulmonary artery to the aorta) allows blood to bypass the narrowed segment. When this vessel closes naturally after birth, the full obstruction is unmasked and blood flow to the lower body drops. Babies may become lethargic, feed poorly, develop fast or laboured breathing, and appear pale or mottled. This is a medical emergency, and a medication called prostaglandin E1 (alprostadil) is given intravenously to reopen the ductus arteriosus as a life-saving bridge while surgical repair is arranged.
In older children with a milder narrowing, the condition may go unnoticed for months or years. The body develops collateral blood vessels, smaller arteries that grow to carry blood around the obstruction, which can partially compensate for the narrowing. These children may be entirely well and active, with the coarctation only discovered when a doctor detects a heart murmur, notices that blood pressure in the arms is higher than expected, or finds that the pulses in the legs are weak or difficult to feel. Some older children report headaches, leg aching or cramps during exercise, reduced stamina compared to their peers, or nosebleeds. High blood pressure detected during a routine check is one of the most common ways that coarctation is picked up in school-age children and teenagers.
🟢 Usually not concerning
🟡 Worth medical review
🔴 Seek urgent assessment
The classic diagnostic clue is a difference in blood pressure between the upper and lower body. When blood pressure measured in the arms is significantly higher than blood pressure measured in the legs (typically a gradient of 20 mmHg or more), coarctation should be suspected. Weak or absent pulses in the groin (femoral pulses) are another important finding on clinical examination, and a heart murmur may also be heard.
The key diagnostic investigation is an echocardiogram, a painless ultrasound scan of the heart and aorta. Dr Giardini performs and interprets all echocardiograms personally, allowing the narrowing to be visualised directly, its severity assessed, the left ventricle examined for thickening, and any associated conditions (such as a bicuspid aortic valve or VSD) identified. Results are available immediately and can be discussed during the same appointment.
An electrocardiogram (ECG) is usually performed to check for signs of left ventricular hypertrophy. In older children and teenagers, or when the anatomy of the aortic arch is complex, a cardiac MRI or CT scan provides detailed three-dimensional images of the aorta and is particularly valuable for planning treatment. MRI has the advantage of using no ionising radiation and also allows blood flow and pressure gradients to be measured non-invasively, making it an excellent tool for both diagnosis and long-term follow-up.
In most cases, yes, although the urgency and approach depend on the severity.
A mild narrowing with normal blood pressure, no significant gradient between the arms and legs, and no evidence of left ventricular strain may be managed with careful monitoring and regular follow-up. However, if the gradient increases over time or blood pressure becomes elevated, treatment is recommended.
Significant coarctation, whether causing symptoms in a newborn or producing elevated blood pressure and a measurable gradient in an older child, is treated to relieve the obstruction, normalise blood pressure, reduce the workload on the heart and prevent long-term complications. The aim of treatment is to restore unobstructed blood flow through the aorta.
The choice of treatment depends on the child's age, weight, the anatomy of the narrowing and whether associated heart defects are present.
Surgical repair is the standard treatment for newborns and young infants with significant coarctation. The operation is performed through an incision on the left side of the chest (not through the breastbone) and does not require a heart-lung bypass machine. The most common technique is resection and extended end-to-end anastomosis, in which the narrowed segment is removed and the two healthy ends of the aorta are joined back together. Other surgical approaches include the subclavian flap repair, in which tissue from the subclavian artery is used to widen the narrowed area, and patch aortoplasty, in which a patch of synthetic material or the patient's own tissue is used to enlarge the aorta. The choice of technique depends on the individual anatomy. Surgical outcomes are excellent, with very low complication rates and rapid recovery.
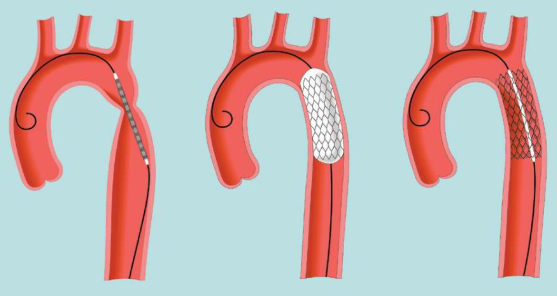
Catheter-based treatment (balloon angioplasty with or without stent placement) is more commonly used in older children, teenagers and in cases of re-coarctation (recurrence of the narrowing after previous repair). During this procedure, a thin catheter is inserted through a blood vessel in the leg and guided to the narrowed segment. A balloon at the tip of the catheter is inflated to widen the aorta, and in older children a stent (a small metal tube) may be placed to hold the artery open. This approach avoids open surgery, requires a shorter hospital stay, and has excellent success rates. Stents used in growing children can be re-dilated at a later stage if needed as the child grows.
Medical treatment with prostaglandin E1 is used as an emergency measure in critically unwell newborns to reopen the ductus arteriosus and restore blood flow to the lower body while surgical repair is arranged. This is not a definitive treatment but a vital bridge to surgery.
Most children recover quickly after coarctation repair and return to normal activities. Surgical patients are typically in hospital for about a week, while those who undergo catheter-based treatment often go home within a day or two. Symptoms such as leg aching, headaches and reduced exercise tolerance usually resolve promptly once the obstruction is relieved.
However, lifelong follow-up is essential, and this is one of the most important messages for parents to understand. Even after a technically successful repair, children with coarctation require regular monitoring for several reasons.
Blood pressure can remain elevated or become elevated again over time, even when the anatomical repair is excellent. The prevalence of long-term hypertension in patients who have had coarctation repair is reported at 25 to 68%, depending on the age at repair and the length of follow-up. Blood pressure should be measured in both the arms and legs at every follow-up visit, and ambulatory blood pressure monitoring (ABPM) over 24 hours is a valuable tool for detecting hypertension that may not be apparent during a clinic appointment. Children who are treated earlier in life tend to have a lower risk of long-term hypertension.
Re-coarctation (recurrence of the narrowing) occurs in approximately 5 to 10% of cases, depending on the surgical technique, the age at repair and the anatomy. This is why periodic imaging of the aorta, whether by echocardiography, MRI or CT, is part of the routine follow-up programme.
The aortic valve also needs monitoring, particularly in children with a bicuspid valve, as it may develop stenosis or regurgitation over the years. In rare cases, aneurysms (areas of widening) can develop at the repair site or elsewhere in the aorta, and there is a small but recognised risk of cerebrovascular complications related to the abnormal blood vessel architecture that can accompany coarctation. Regular follow-up allows all of these to be detected and managed early.
This is one of the most common questions parents ask, and the answer is encouraging. After successful repair with normal blood pressure and no residual narrowing, most children can participate fully in physical activity and sport. Dr Giardini has particular expertise in sport cardiology and can provide individualised exercise guidance based on your child's anatomy, blood pressure profile and cardiac function. Some children with residual gradients, elevated blood pressure or aortic arch abnormalities may be advised to avoid very high-intensity isometric activities (such as heavy weightlifting), but most recreational and competitive sport is possible.
The long-term outlook for children with treated coarctation is very good. Modern surgical and catheter-based techniques achieve excellent anatomical results, heart function returns to normal, and most children grow and develop without restriction. Life expectancy in patients treated in childhood is approaching that of the general population, particularly when repair is performed early and blood pressure is well controlled.
The key to the best possible outcome is early diagnosis, timely treatment and consistent lifelong follow-up. Dr Giardini works closely with families to ensure that every child receives the right treatment at the right time and that long-term monitoring is in place to catch and address any issues before they cause problems. If you have concerns about your child or would like to arrange an assessment, please do not hesitate to contact Dr Giardini's team to book an appointment.
It can be, particularly in newborns when the narrowing is severe and presents as an emergency. In many children, however, the condition is milder and very treatable. With appropriate care, outcomes are excellent and most children lead completely normal lives.
Yes. Mild coarctation may not be apparent at the newborn check because the ductus arteriosus is still partially open and masking the obstruction. Some cases are only diagnosed later in childhood when a murmur, high blood pressure or weak leg pulses are detected.
This depends on the severity and the child's age. Newborns and young infants with significant coarctation are usually treated surgically. Older children and teenagers may be suitable for catheter-based treatment with balloon angioplasty and stenting. Dr Giardini will advise on the most appropriate option.
Re-coarctation occurs in up to 20% of cases. This is one of the key reasons why lifelong follow-up with regular imaging and blood pressure checks is essential.
In most cases, yes. After successful repair with normal blood pressure and no residual obstruction, most children can participate fully in sport. Dr Giardini provides individualised exercise advice based on each child's specific situation.
The narrowing increases resistance to blood flow, causing pressure to build up above the obstruction (in the head, arms and upper body) while blood flow and pressure below it (to the kidneys, abdomen and legs) are reduced.
The anatomical narrowing can be treated very effectively, but the condition requires lifelong follow-up because blood pressure can remain or become elevated after repair, and the aorta and aortic valve need monitoring over time.
Yes. Up to 50 to 85% of children with coarctation also have a bicuspid aortic valve. It can also occur alongside ventricular septal defects, patent ductus arteriosus and other congenital heart conditions, which is why a comprehensive cardiac assessment is important.
In newborns with critical coarctation, treatment is urgent. In older children with a less severe narrowing, treatment is planned carefully and is rarely an emergency. Dr Giardini will help you understand the appropriate timeline for your child.
If your child has been diagnosed with coarctation, has unexplained high blood pressure, a heart murmur has been detected, or if weak leg pulses have been noticed, specialist assessment is recommended. Dr Giardini can provide a definitive diagnosis with same-day echocardiography and a clear management plan.
In coarctation of the aorta, the narrowing reduces blood flow to the lower part of the body. This means the pulses in the legs (femoral pulses) can feel weaker or delayed compared to the arms. This is often one of the key clinical signs that leads to the diagnosis.
Yes, it can. Because blood pressure is higher in the upper body, some children and teenagers may develop headaches or occasional nosebleeds. These symptoms are not specific on their own, but when combined with high blood pressure they can be an important clue.
Yes. Many milder cases are diagnosed later in childhood during routine health checks, sports screening or GP visits. A murmur, high blood pressure, or a difference between arm and leg pulses may lead to referral for further assessment.
Author: Dr. Alessandro Giardini, MD, PhD
Written 03/04/2026