
Dr. Alessandro Giardini
If you have been told that your child has a ventricular septal defect, or a "hole in the heart," it is completely natural to feel concerned. The reassuring news is that a VSD is the most common congenital heart defect in children, and the vast majority do very well. Many small VSDs close on their own without any treatment at all, and even when intervention is needed, the results are excellent. In North America and Europe, elective VSD repair carries a mortality rate below 1%, and most children go on to live completely normal, active lives.
A key part of specialist assessment is understanding whether your child's VSD simply needs monitoring or whether it is causing the heart to work harder and may benefit from treatment. Dr Giardini will guide you through this clearly during your consultation.
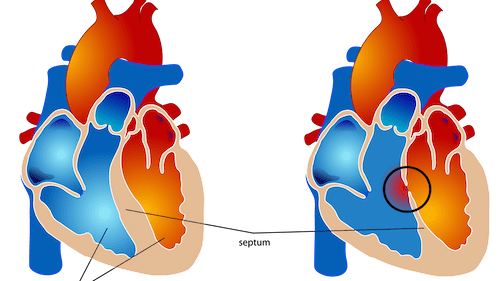
The heart has four chambers. The two lower chambers, called the ventricles, do the main pumping work. They are normally separated by a solid wall known as the ventricular septum. A VSD is a hole in this wall.
In a normal heart, the left ventricle pumps oxygen-rich blood out to the body, while the right ventricle pumps oxygen-poor blood to the lungs. With a VSD, some oxygen-rich blood from the left ventricle passes through the hole into the right ventricle and is pumped back to the lungs unnecessarily. This means the lungs receive more blood than they need, and the left side of the heart has to work harder to keep up with the body's demands.
The impact of this extra blood flow depends almost entirely on the size and position of the hole. A tiny VSD may allow only a trickle of blood across and cause no strain on the heart at all. A large VSD can allow a significant volume of blood to recirculate through the lungs, leading to symptoms in the first weeks of life.
A VSD develops early in pregnancy during the critical period when the heart is forming from a simple tube into four separate chambers. If the wall between the ventricles does not close completely during this process, a hole remains. In the vast majority of cases, there is no identifiable cause and nothing a parent did or did not do played any role.
In some children, a VSD may be associated with a genetic condition or chromosomal abnormality, and occasionally it can run in families. However, most VSDs occur as isolated findings in otherwise healthy babies. If there is any concern about a genetic association, further testing can be discussed during your consultation.
VSDs are classified by their position in the ventricular septum, and this matters because the location influences whether the defect is likely to close on its own and which treatment approach is most suitable.
Perimembranous VSDs are the most common type, accounting for around 80% of all cases. They occur in the upper, membranous portion of the septum, close to the aortic and tricuspid valves. Some perimembranous VSDs reduce in size over time as tissue from the tricuspid valve forms a pouch that partially or completely covers the hole. However, because of their proximity to the valves and the heart's electrical conduction system, these defects require careful monitoring.
Muscular VSDs occur within the muscular body of the septum and are the type most likely to close spontaneously, particularly during the first year or two of life. They rarely require treatment unless they are large.
Outlet (supracristal) VSDs sit just below the pulmonary valve in the upper part of the septum. These are less common overall but occur more frequently in children of East Asian heritage. They rarely close on their own and can sometimes cause the aortic valve to prolapse over time, which is why they tend to be referred for repair even when they are small.
Inlet VSDs are located near the tricuspid and mitral valves in the lower part of the septum. These are associated with atrioventricular septal defects and generally do not close spontaneously.
The type and location of your child's VSD will be explained clearly during the consultation.
Many children with a VSD have no symptoms at all, and this is an important point for parents to understand. A small VSD typically causes nothing more than a heart murmur, a "whooshing" sound that the doctor can hear with a stethoscope during a routine examination. Children with small VSDs grow and develop normally, are fully active and do not need any restrictions.
When symptoms do occur, they are related to the volume of extra blood flowing through the lungs and the extra work the heart has to do. Babies with a moderate or large VSD typically begin to show signs from around four to six weeks of age, as the natural resistance in the lung blood vessels falls after birth and the amount of blood crossing the defect increases. Symptoms may include fast or laboured breathing, tiring easily during feeds, sweating during feeding, poor weight gain, a pale or mottled appearance and frequent chest infections. These symptoms reflect the heart working harder than it should and some fluid accumulating in the lungs, a condition sometimes referred to as heart failure in infancy.
Older children with a significant VSD that has not been treated may experience breathlessness during exercise and reduced stamina compared to their peers, although this presentation is much less common because most large VSDs are identified and managed in infancy.
🟢 Usually not concerning
🟡 Worth medical review
🔴 Seek prompt assessment
Most VSDs are first suspected when a doctor hears a heart murmur during a newborn check or a routine postnatal examination. The murmur is caused by the turbulent flow of blood passing through the hole and is often quite loud even when the defect is small.
The key diagnostic test is an echocardiogram, a painless ultrasound scan of the heart. Dr Giardini performs and interprets all echocardiograms personally, allowing him to confirm the diagnosis, identify the exact position and size of the defect, measure how much blood is crossing from left to right, assess whether the left side of the heart is enlarged, and check the heart valves and other structures. Findings can be discussed with you during the same appointment.
An electrocardiogram (ECG) is usually performed alongside the echocardiogram to assess the heart's electrical activity. In selected cases, particularly when there is concern about elevated pressures in the lungs or when the clinical picture does not match the echocardiographic findings, a cardiac catheterisation may be recommended to measure pressures directly.
A key part of Dr Giardini's consultation is explaining clearly whether the VSD is small and safe to monitor, whether it is likely to close on its own, or whether the heart is showing signs of strain that may warrant treatment.
Not always, and this is often the most reassuring part of the consultation for parents. Many small VSDs never require any intervention at all. Muscular VSDs in particular have a high rate of spontaneous closure during the first two years of life, and even many perimembranous VSDs become smaller over time.
For children with a small, haemodynamically insignificant VSD, the only requirement is periodic follow-up with echocardiograms to confirm the defect is not causing any strain on the heart and to watch for any changes in the nearby valves. These children can lead completely normal lives with no activity restrictions.
Treatment is considered when the VSD is large enough to cause symptoms, when the baby is failing to gain weight adequately despite nutritional support, or when there is clear evidence of left heart enlargement or increased blood flow to the lungs on the echocardiogram. The aim of treatment is to prevent long-term damage to the heart and lungs.
When treatment is needed, the approach depends on the size and location of the defect and on the child's clinical condition.
Medical management is often used as a first step to stabilise babies while they grow. Diuretic medications (such as furosemide) help the kidneys remove excess fluid from the body, easing the workload on the lungs. High-calorie formula or fortified breast milk may be recommended to support weight gain in babies who are finding it difficult to feed. Medication alone will not close a VSD, but it can buy valuable time if the baby needs to grow before surgery can be performed safely.
Surgical closure is the standard treatment for most VSDs that require repair. The operation is performed under general anaesthetic using a heart-lung bypass machine. The surgeon closes the hole either with direct stitches (for smaller defects) or, more commonly, with a small patch made of synthetic material or tissue from the lining around the heart (pericardium). The heart's own tissue grows over the patch, sealing it permanently. Surgery is usually performed within the first three to six months of life for babies with significant symptoms, although the timing depends on the individual child's condition and weight. The success rate of VSD surgery is very high, recovery typically requires only a few days in hospital, and most babies show an immediate improvement in feeding and weight gain.
Catheter-based closure is an option for a smaller number of VSDs, most commonly muscular defects that are difficult to reach surgically. A closure device is delivered through a catheter inserted via a vein in the leg and positioned across the hole under ultrasound and X-ray guidance. Transcatheter closure of perimembranous VSDs is technically feasible but is approached with caution because of a recognised risk of damage to the heart's conduction system, which can cause heart block. Whether catheter closure is appropriate depends on the individual child's anatomy and will be discussed during the consultation.
Children with a VSD have a small risk of developing endocarditis, an infection of the inner lining of the heart caused by bacteria entering the bloodstream. Good dental hygiene, including regular brushing, flossing and routine dental visits, is the most important way to reduce this risk. In most cases, antibiotics before dental procedures are not routinely required, although they may be recommended for the first six months after surgical or device closure. Whether endocarditis precautions apply to your child will be discussed during the consultation.
Small VSDs that do not cause right or left heart enlargement generally pose no long-term risk. Many persist as tiny holes with a murmur but cause no functional problems throughout life.
Larger untreated VSDs, however, can cause progressive damage over time. The sustained extra blood flow through the lungs can lead to pulmonary hypertension (high pressure in the lung blood vessels), which, if severe and prolonged, may eventually become irreversible, a condition known as Eisenmenger syndrome. Untreated large VSDs can also lead to heart failure and, in later life, heart rhythm disturbances. This is why timely assessment and, when indicated, early repair are so important, and why Dr Giardini recommends closing significant defects during infancy rather than waiting for complications to develop.
The outlook for children with a VSD is excellent. Many small defects close spontaneously and require no treatment at all. Children who undergo surgical repair in infancy can expect a normal lifespan and a normal quality of life with no restrictions on physical activity. After a successful repair, the heart generally returns to a completely normal state.
Children with small VSDs that do not close but remain haemodynamically insignificant also do very well. They may continue to have a heart murmur, but this does not affect their health or their ability to participate fully in sport and everyday life. Dr Giardini will arrange appropriate long-term follow-up to ensure the heart remains healthy and the valves near the defect are not affected over time.
If you have any questions about your child's VSD or would like to arrange an assessment, please do not hesitate to contact Dr Giardini's team to book an appointment.
In most cases, no. Small VSDs are harmless and often close on their own. Larger VSDs may need treatment, but with appropriate care the outcomes are excellent and the vast majority of children live completely normal lives.
Yes. Many small VSDs, particularly muscular defects, close spontaneously during the first one to two years of life. Some perimembranous VSDs also reduce in size over time. Dr Giardini will monitor your child to track whether this is happening.
In babies, the most important signs are fast or laboured breathing, tiring or sweating during feeds, poor weight gain and frequent chest infections. These typically appear from around four to six weeks of age if the VSD is large.
Not always. Many children with a VSD never need surgery. When it is required, typically for larger defects causing symptoms or heart strain, the operation is very safe and the results are excellent.
Babies with large, symptomatic VSDs are usually treated within the first three to six months of life. Smaller defects that are not causing problems are monitored, and some close on their own by the age of two to four.
Most children with a small VSD or a successfully repaired VSD can participate fully in sport and physical activity with no restrictions.
Both are holes in the heart, but they are in different locations. A VSD is in the wall between the lower pumping chambers (ventricles), while an ASD is in the wall between the upper filling chambers (atria). VSDs are more common and more likely to cause symptoms in infancy.
In most cases, routine antibiotic prophylaxis is not required. However, it may be recommended for the first six months after VSD closure. Good dental hygiene is the most effective way to prevent endocarditis.
Eisenmenger syndrome is a rare but serious complication of a large, untreated VSD. Over many years, the sustained extra blood flow damages the lung blood vessels, eventually causing irreversible high pressure that reverses the direction of the shunt. This is preventable with timely VSD repair.
If your child has been diagnosed with a VSD, or if a heart murmur has been detected, specialist assessment is recommended. Dr Giardini can determine the type and size of the defect, explain its significance, and advise on whether monitoring or treatment is needed.
Author: Dr. Alessandro Giardini, MD, PhD
Written 03/05/2026